
GLP-1 receptor agonists — semaglutide (Ozempic, Wegovy), tirzepatide (Mounjaro, Zepbound), and related agents — have become among the most prescribed medications in the United States, driven by their efficacy for type 2 diabetes management and weight loss. As their use has expanded, hair loss has emerged as a commonly reported side effect, generating substantial patient concern and media coverage under the "Ozempic hair loss" label.
The clinical question is whether GLP-1 drugs cause hair loss directly — through a pharmacological mechanism — or whether the hair loss is secondary to the rapid weight loss these drugs produce. This distinction matters for clinical management: if the hair loss is secondary to weight loss (telogen effluvium), it is likely self-limiting and does not require drug discontinuation; if it is a direct drug effect, the risk-benefit calculation changes.
This analysis reviews the hair loss data from the pivotal GLP-1 trials, examines the proposed mechanisms, and assesses what the evidence supports about the nature and management of GLP-1-associated hair loss.
The Trial Data: What the Pivotal Studies Show
The STEP trial program for semaglutide 2.4 mg (Wegovy) for obesity reported alopecia as an adverse event in approximately 3% of participants versus 1% for placebo in STEP 1 (n=1,961). The SURMOUNT-1 trial for tirzepatide (n=2,539) reported hair loss in approximately 5.7% of participants versus 1% for placebo. These rates are statistically significant versus placebo and represent a real signal — hair loss is more common in GLP-1 drug users than in placebo-treated controls.
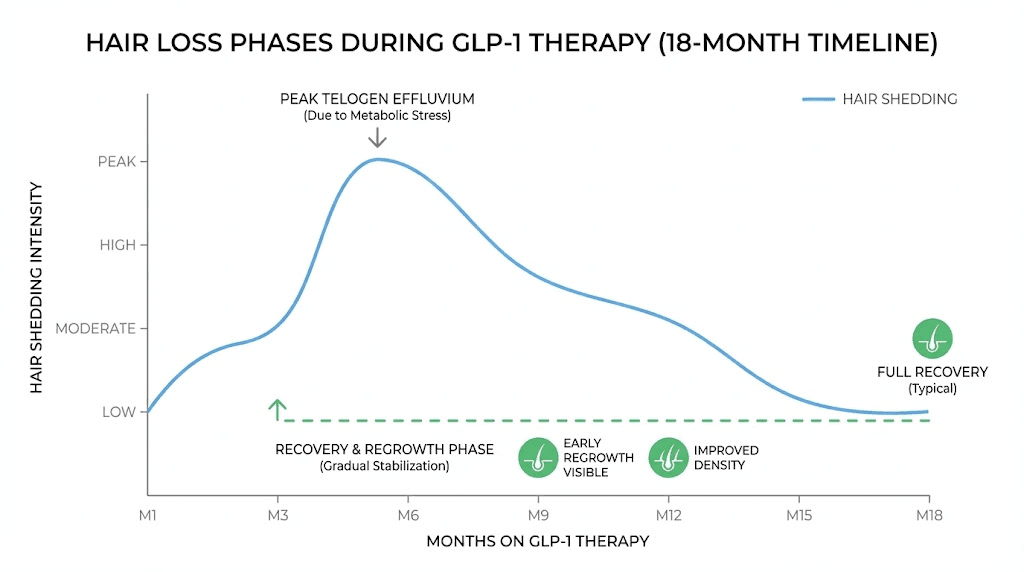
The critical observation from the trial data is the correlation between hair loss and weight loss magnitude. In the STEP trials, hair loss was more common in participants who lost more weight — consistent with telogen effluvium secondary to rapid caloric restriction and weight loss, rather than a direct pharmacological effect of semaglutide. The timing of hair loss onset (typically 2–4 months after initiating treatment, coinciding with the period of most rapid weight loss) is also consistent with TE pathophysiology.
No mechanistic evidence for a direct GLP-1 receptor-mediated effect on hair follicles has been published. GLP-1 receptors are expressed in multiple tissues, but hair follicle expression has not been demonstrated in published studies. The current evidence strongly favors weight-loss-induced TE as the primary mechanism, not a direct drug effect.
The Claim
"Ozempic and other GLP-1 drugs cause hair loss as a direct side effect — the drug itself damages hair follicles, and users should expect significant shedding that may not resolve even after stopping the medication."
(Composite representative claim reflecting media coverage and patient forum discussions of GLP-1-associated hair loss.)
What the Evidence Actually Shows
The evidence supports GLP-1-associated hair loss as a real phenomenon — the trial data show significantly higher rates versus placebo. However, the evidence strongly favors weight-loss-induced telogen effluvium as the mechanism, not direct follicular damage by the drug. This distinction has important clinical implications.
Telogen effluvium secondary to rapid weight loss is well-documented in the bariatric surgery literature, where hair loss rates of 30–50% are reported following gastric bypass — substantially higher than the 3–6% rates seen with GLP-1 drugs, which produce more gradual weight loss. The TE mechanism predicts that hair loss should be self-limiting (resolving within 6–12 months as weight loss stabilizes) and should not require drug discontinuation in most cases.
The claim that GLP-1 drugs "damage hair follicles" and that shedding "may not resolve" is not supported by the current evidence. The trial data do not include long-term hair loss follow-up, but the TE mechanism predicts resolution. Post-marketing surveillance data on long-term hair loss outcomes with GLP-1 drugs are limited as of 2026.
Clinical Management
For patients experiencing hair loss on GLP-1 drugs, the evidence-based approach is: reassurance that the hair loss is likely TE secondary to weight loss and is expected to be self-limiting; evaluation for concurrent nutritional deficiencies (iron, zinc, protein intake) that may exacerbate TE in the context of caloric restriction; and avoidance of unnecessary drug discontinuation based on hair loss alone, given the significant metabolic benefits of these medications.
Adequate protein intake during weight loss is important for minimizing TE severity — protein restriction exacerbates TE, and patients on GLP-1 drugs with reduced appetite may have inadequate protein intake. Monitoring ferritin and zinc levels is reasonable given the potential for nutritional deficiencies during rapid weight loss.
Verdict: Partially Supported
GLP-1-associated hair loss is a real phenomenon supported by trial data showing significantly higher rates versus placebo. The mechanism is most consistent with weight-loss-induced telogen effluvium rather than direct follicular damage. The claim that GLP-1 drugs directly damage hair follicles is not supported by the current evidence. The hair loss is expected to be self-limiting in most cases. Clinical management should focus on nutritional optimization and reassurance rather than drug discontinuation. Evidence rating: 3/5.