This article is Part 2 of a 3-part series on NOVOGRO™, a new category of intentionally designed molecules that target damaged hair follicles from the inside and out. In this installment, we look at NV-1065, a rare non-steroidal, non-hormonal DHT blocker taking aim at finasteride. The core question is straightforward: is this marketing, or science?
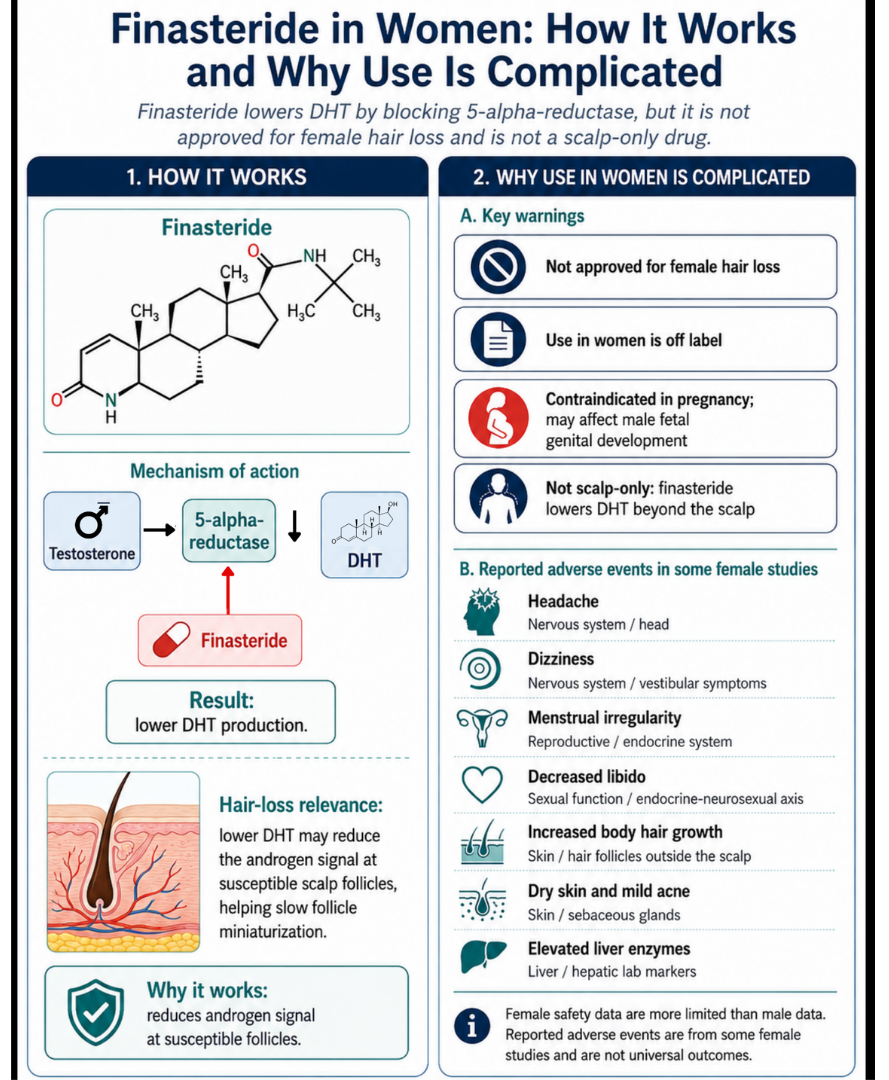
Few treatments have shaped the hair loss field as much as finasteride, most commonly marketed as Propecia or Proscar. Originally developed by Merck & Co. for symptomatic benign prostatic hyperplasia, clinicians later observed hair growth as an unexpected side effect. Finasteride is an irreversible 5-alpha-reductase (5-AR) inhibitor and a steroidal anti-androgen. It works by blocking the conversion of testosterone to dihydrotestosterone (DHT), a central driver of androgen-sensitive follicle miniaturization. In susceptible hair follicles, androgen signaling can shorten anagen, shrink the follicle, and gradually convert thick terminal hairs into thinner, weaker fibers.[1]
In men, finasteride is FDA-approved for androgenetic alopecia at 1 mg/day. However, adverse effects include sexual dysfunction, depression, and breast enlargement. In some men, sexual dysfunction may persist even after stopping the medication, and in rare cases finasteride may complicate early detection of some prostate pathology. The situation is more complex for women. Finasteride is not FDA-approved for female hair loss, the evidence base is smaller, the dosing is different, and it is classified as pregnancy category X, meaning it must not be taken by women who are or may become pregnant because of developmental risks to male fetuses. Despite this, finasteride is still used off-label in women with female pattern hair loss.[2]
Recently, our team came across a new non-steroidal 5-AR inhibitor called NV-1065, a molecule within the NOVOGRO™ complex (the technology behind RE:YOU). That raises the central question of this article: can DHT-related follicle miniaturization in women be addressed without relying on a drug with significant systemic adverse effects? This breakdown examines the female evidence for finasteride and compares it to an emerging, non-steroidal anti-androgen strategy.
How Finasteride Works
Mechanistically, finasteride inhibits type II 5-AR, blocking the conversion of testosterone into DHT. These enzymes help generate DHT within the skin and around the hair follicles. In men with androgenetic alopecia, balding scalp contains miniaturized follicles and higher DHT compared with non-balding scalp, and finasteride decreases both scalp and serum DHT concentrations. A 1 mg oral dose suppresses serum DHT rapidly, reaching roughly 65-70% suppression within 24 hours.[1]
| Why it matters | Finasteride’s clinical strength |
|---|---|
| Targets DHT production | DHT is one of the best-established androgen signals involved in follicle miniaturization. |
| Acts upstream | It interferes with DHT formation before DHT binds androgen-sensitive follicle pathways. |
| Has long-standing clinical use | Finasteride 1 mg is indicated for male pattern hair loss, while higher-dose finasteride is used for prostate indications. |
| Produces measurable endocrine effects | Its efficacy comes from changing a hormone pathway, not simply conditioning the scalp. |
Its weaker point lies in the female evidence base. The most important randomized controlled trial studied 137 postmenopausal women ages 41 to 60 with androgenetic alopecia. Participants received either finasteride 1 mg daily or placebo for 12 months. The trial found no meaningful improvement in hair count, patient or investigator assessment, global photography, or scalp biopsy measures compared with placebo. Higher doses have shown more encouraging signals, but the evidence is less definitive. A 2023 systematic review of oral and topical finasteride in women found that 10 of 14 included studies reported a high rate of recovery or improvement, and suggested that 5 mg oral finasteride may be effective in some normoandrogenic women with female pattern hair loss.[3][4]
This unresolved dosing question compounds safety uncertainty. Higher dosing could plausibly increase side effect risk, yet no randomized trial has directly compared doses in women to establish the optimal dose or its corresponding safety profile. Much of the signal comes from open-label, uncontrolled, retrospective, or small studies rather than large placebo-controlled trials.
Side Effects of Finasteride Use in Women
Finasteride’s side effect profile is the most important clinical consideration. It does not act solely on the scalp. It inhibits a hormone-conversion pathway present across multiple tissues throughout the body. In women, finasteride remains less thoroughly characterized than in men because the research base is smaller, and pregnancy category X remains the major safety constraint. This is why most studies have focused on postmenopausal women or on women using reliable contraception.
Beyond teratogenicity, reported adverse effects in women include menstrual irregularities, decreased libido, breast tenderness, mood changes, and headaches, though incidence rates vary across trials and observational cohorts. For a more detailed breakdown, see our article Finasteride for Female Hair Loss: What the Evidence Supports.[5]
Ultimately, these data expose a fundamental problem: finasteride is not a scalp-only intervention. It is a systemic hormonal drug that alters endocrine biology throughout the body. That is why its use in women requires careful diagnosis, strict pregnancy-risk management, and continuous medical supervision, and why the field has kept searching for a non-steroidal DHT inhibitor that could preserve follicle-protection benefits without the same systemic costs.
NV-1065: A Non-Steroidal Alternative?
The Claim
“NV-1065 targets DHT-driven follicle miniaturization using a non-steroidal, scalp-friendly molecule.”
(Composite representative claim; reflects NV-1065’s proposed positioning as a non-steroidal DHT inhibitor targeting the environment around the hair follicle.)
What the Evidence Actually Shows
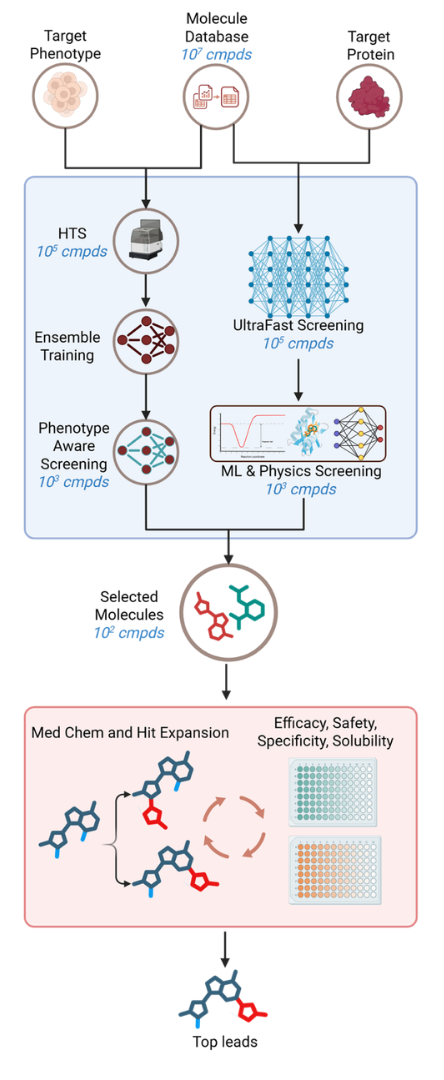
NV-1065 enters the conversation from the opposite starting point. Rather than repurposing a drug with known systemic side effects, an interdisciplinary research group set out to develop a novel non-steroidal 5-AR inhibitor from the ground up. The team combined expertise spanning medicinal chemistry, physiology, and computational chemistry, and used machine learning to screen millions of compounds for structural and chemical properties consistent with selective 5-AR inhibition.
In their workflow, large libraries of candidate molecules were computationally screened against 5-AR using a multi-parameter ranking system. Candidates were scored on predicted target interaction, scalp compatibility, non-drug-like properties, dermal penetration potential, and off-target risk. The highest-ranked candidates were then validated in vitro against human 5-AR enzymes and subjected to dozens of safety studies in primary human skin and non-skin cell models.
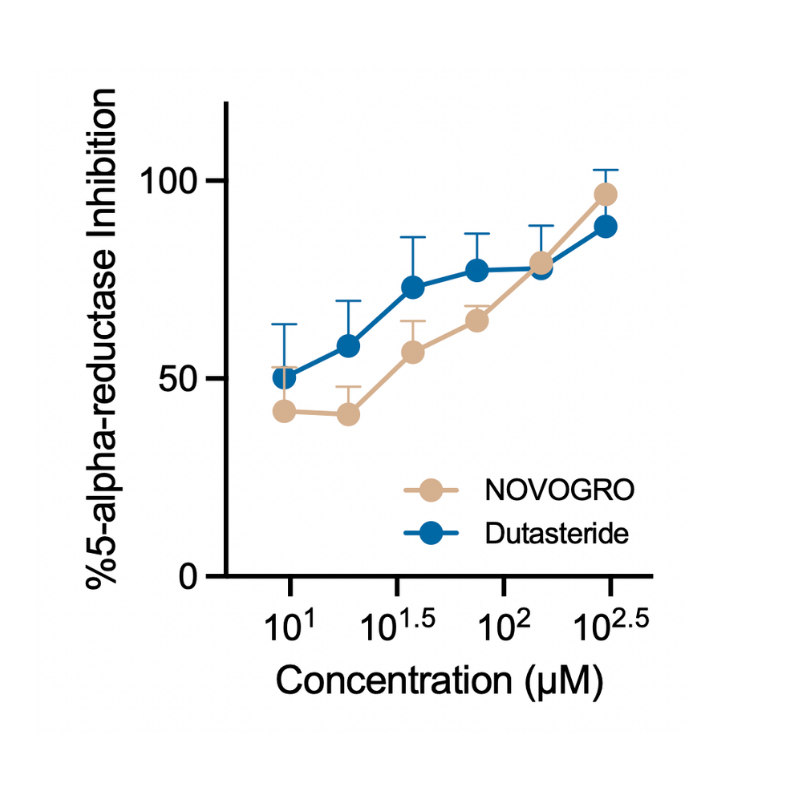
The research group developed an in-house tool to test 5-AR activity and reported that NV-1065 achieved human 5-AR inhibition comparable to dutasteride, finasteride’s stronger cousin. That is a high bar. NV-1065 also appears to be a relatively small molecule, around 250 g/mol, which suggests it should not have major difficulty penetrating the scalp and reaching the region around the hair follicle. The group also reported that an earlier, less soluble molecule was optimized into a water-compatible version suitable for serum use. Importantly, they showed that NV-1065 was non-mutagenic, non-sensitizing, and non-toxic across a large battery of safety tests involving primary human skin and non-skin cells.
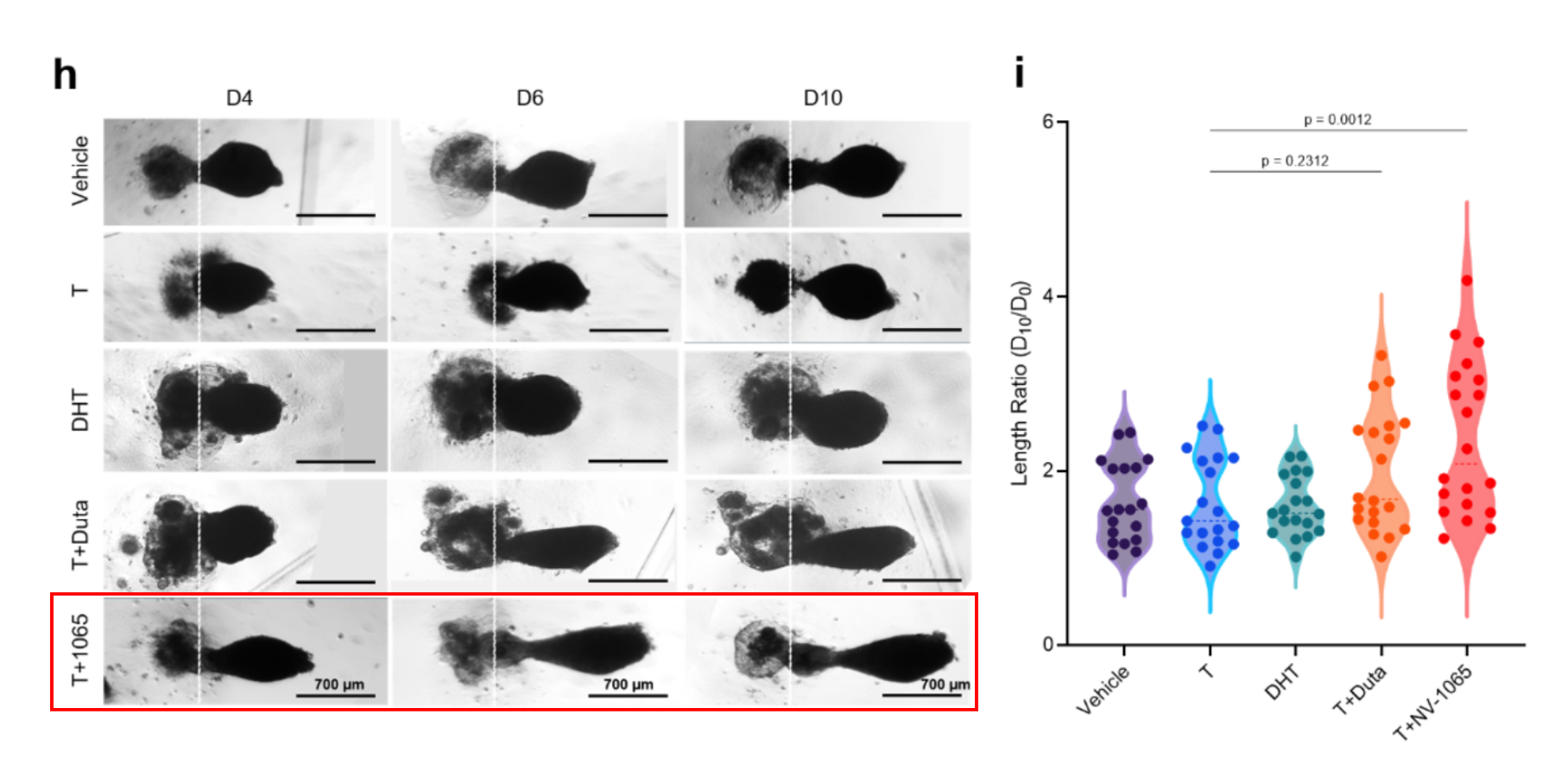
In a series of experiments, the researchers tested NV-1065 in a 3D hair follicoid model. A hair follicoid is a small lab-grown mini hair follicle created by combining keratinocytes and dermal papilla cells in a 3D gel, where they self-organize into a spherical structure and sprout a hair peg-like extension over about 10 days.[6] In this model, DHT or testosterone prevented the follicoid from sprouting. Dutasteride rescued that effect, but NV-1065 was reported to be about 34.3% more effective than dutasteride at counteracting testosterone- or DHT-related miniaturization stress.[6]
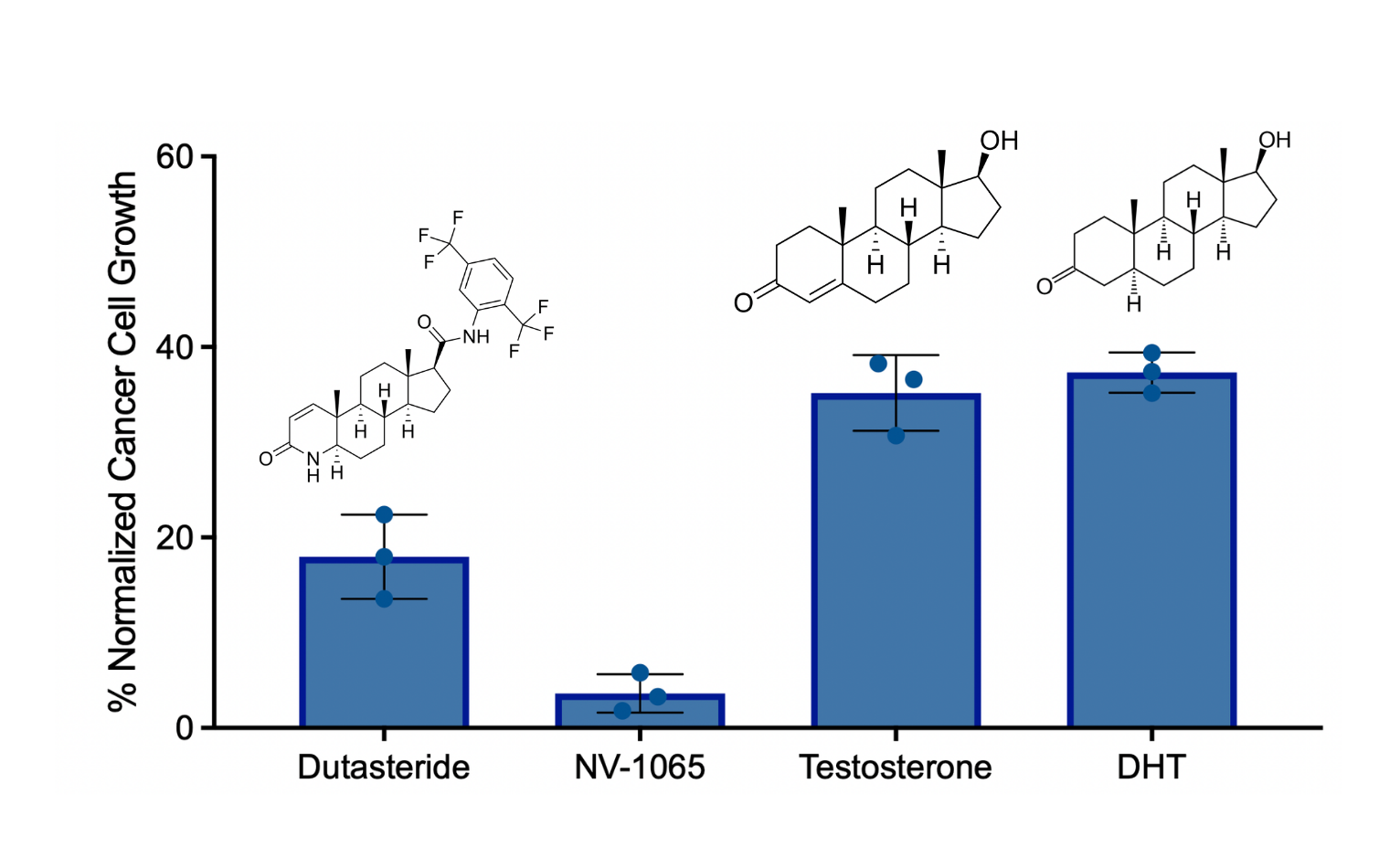
In another experiment, the researchers compared the effects of steroids such as testosterone, finasteride, and dutasteride on steroid-responsive tumor cells. The steroidal compounds promoted growth, whereas NV-1065 did not show the same steroidal growth response, which the authors use to support the claim that NV-1065 is structurally non-hormonal.
Overall, the evidence package presented in the NOVOGRO™ study is stronger than what we typically see for emerging DHT blockers in this category. Our editorial team also notes that the researchers reported an ongoing clinical study involving more than 150 participants.
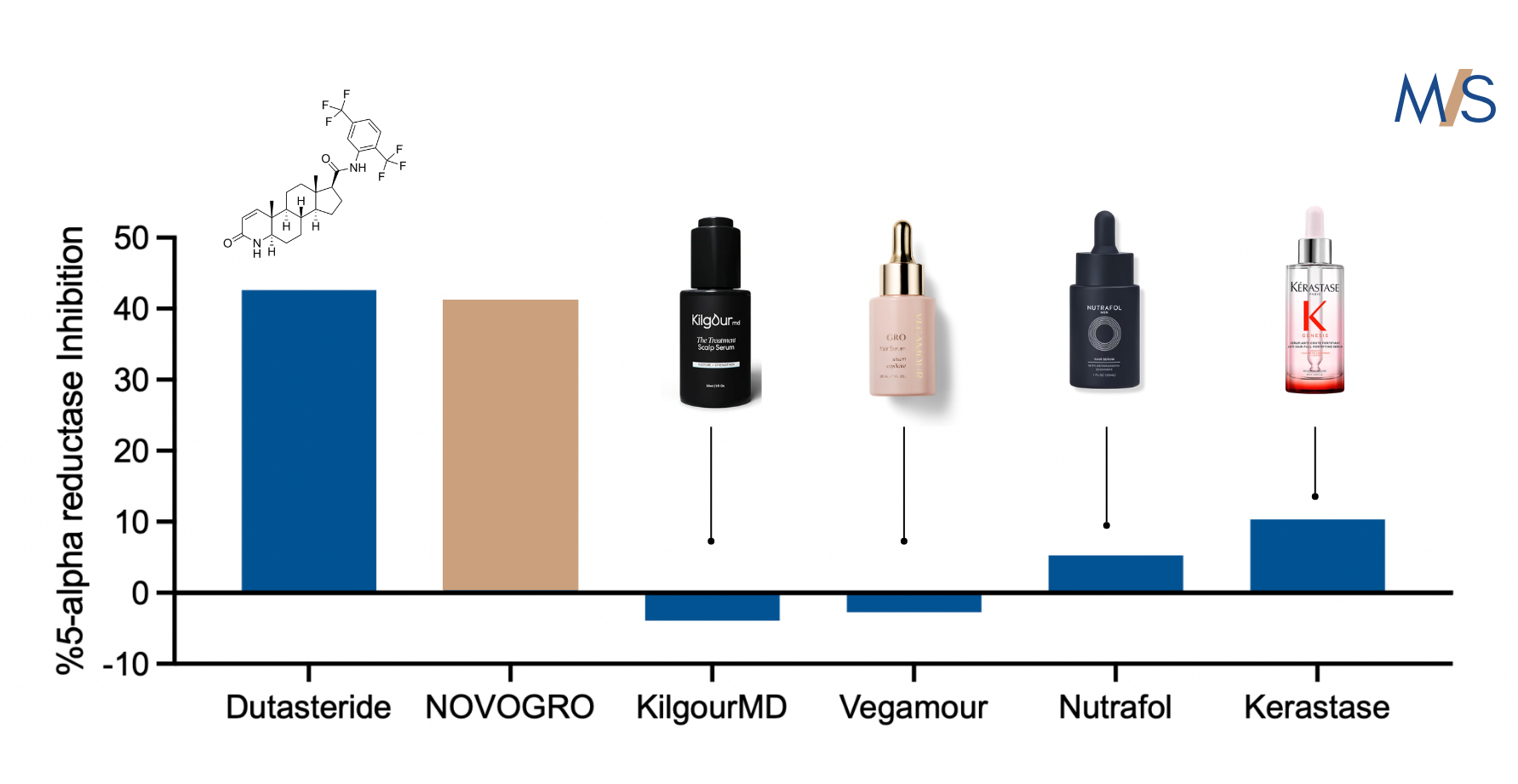
Motivated by the researchers' findings, our team reached out to the researchers to obtain NV-1065, which they kindly provided. After obtaining the molecule, our team was able to replicate their results using their same methodology (Arbor Assays kit). Similarly, we evaluated a number of commercially-available hair thinning formulas and also observed that of four popular serums tested, only one showed a very minor capacity for 5-AR inhibition capacity (Keratase).
NOVOGRO™: Targeting Multiple Complementary Paths
The researchers also describe three additional molecules within NOVOGRO™, NV-273, NV-623, and NV-624, designed to target complementary mechanisms involved in follicle miniaturization, thinning, and hair loss. Their broader thesis is that a multi-pathway approach is necessary for a condition as complex and biologically layered as hair thinning.
For more on the rest of the platform, see:
- Part 1: Minoxidil vs. NOVOGRO™
- Part 3: PP405 vs. NOVOGRO™ (coming soon)
We will update this article as clinical data and any additional mechanistic or safety data become public.
Finasteride vs. NV-1065: The Breakdown
| Category | Finasteride / Dutasteride | NV-1065 |
|---|---|---|
| Original development path | Developed from endocrine and prostate medicine, later used for hair loss. | Developed specifically around hair follicle biology. |
| Primary target | 5-alpha-reductase | 5-alpha-reductase |
| Chemical class | Steroidal compound, specifically a synthetic 4-azasteroid. | Non-steroidal, scalp-penetratable small molecule. |
| Mechanistic approach | Systemic 5-AR inhibition with oral and topical use, reducing DHT through direct enzyme blockade. | Targeted modulation of 5-AR activity with a non-steroidal design intended to minimize broader hormonal effects. |
| Formulability | Poorly water-soluble, often requiring advanced formulation work. | Highly water-soluble and compatible with water-based serums. |
| Side effect profile | Side effects align with endocrine pathway disruption, including libido changes, menstrual changes, and broader systemic concerns in some reports. | Designed for safety, with robust preclinical safety data in human skin and non-skin cells. Long-term safety and real-world follow-up are still needed. |
| Use in women | Pregnancy contraindication, off-label use, and systemic hormone-pathway effects require medical supervision. | Positioned as a non-hormonal alternative, but clinical confirmation is still pending. |
| Clinical data | Mixed in women. Finasteride 1 mg failed in a major postmenopausal trial, while higher doses have shown signals in smaller or less controlled studies. | Randomized clinical study reportedly underway. |
| MoS assessment | Reasonable only for select women under detailed medical supervision. | A new non-steroidal strategy with unusually strong preclinical evidence. |
Verdict: Promising — Awaiting Clinical Data
Finasteride has unquestionably played a pivotal role in the treatment of male androgenetic alopecia and has deepened the field’s understanding of follicle biology. In women, however, the evidence base remains meaningfully constrained by limited efficacy data, pregnancy risk, contraception requirements, systemic endocrine effects, and long-term tolerability concerns. NOVOGRO™, specifically NV-1065, represents a fundamentally different strategy: non-steroidal molecules engineered around DHT-related follicle biology and designed to reduce androgen pressure at the follicle while minimizing broader endocrine exposure. The direction is scientifically interesting and unusually well-supported for a non-RCT evidence package, but the clinical question is not settled until randomized human data arrive.
Preclinical strength: 5/5. Clinical strength: TBD.
References & Further Reading
- U.S. Food and Drug Administration. (2012). PROPECIA (finasteride) tablets for oral use: prescribing information.
- Editorial Team. (2026). Hair Loss Treatments in Women vs. Men: What the Evidence Actually Shows. Marketing or Science.
- Price, V. H., Roberts, J. L., Hordinsky, M., et al. (2000). Lack of efficacy of finasteride in postmenopausal women with androgenetic alopecia. Journal of the American Academy of Dermatology.
- Suchonwanit, P., Iamsumang, W., & Rojhirunsakool, S. (2023). A systematic review of clinical trials using single or combination therapy of oral and topical finasteride in women with pattern hair loss. Advances in Clinical and Experimental Medicine, 32(7), 813.
- Dr. Stella Cho. (2026). Finasteride for Female Hair Loss: What the Evidence Supports (and What It Doesn’t). Marketing or Science.
- Kageyama, T., Miyata, H., Seo, J., Nanmo, A., & Fukuda, J. (2023). In vitro hair follicle growth model for drug testing. Scientific Reports, 13, 4847.